In the Big Taping Truth Trial, we’re looking at the effect of mouth taping on various sleep metrics.
As we gather more data over time, our confidence in the results gets stronger.
At this point in time, we’ve got over 1000 nights of data across 80+ participants, which officially makes us the largest randomized controlled trial on mouth taping! And it’s not over yet – we’re still actively gathering data and recruiting participants. Still, we wanted to share some early findings.
We’re doing something fairly unorthodox here by sharing ongoing results openly. Some may worry that releasing ongoing results could influence future participants’ expectations, which is a valid concern. However, we believe the benefits of openness outweigh that risk, especially since much of our data comes from objective measurements and participants have expectations about taping regardless. Letting people follow along in real time makes the process more transparent and engaging.
Analysis Approach
For each individual, we calculated their average change in each metric (vertical taping versus mustache taping, the control condition). For this analysis, we only included individuals with at least 3 nights per treatment.

For each metric, we consider 3 comparisons: Is vertical (mouth taping) significantly better than mustache (control) for all participants? Is vertical better if we look only at suspected nose breathers? How about only suspected mouth breathers? The bar plot for each metric reflects these three comparisons.
But wait – how do we know who is a “suspected mouth breather”? Well, in our onboarding form, we ask a series of questions that help us guess. We’ll reveal the details of that later.
You may also notice that the numbers in some charts don’t add up to the total number of participants — that’s because a few people (~12%) didn’t fully complete the onboarding survey, so we couldn’t confidently categorize them as mouth or nose breathers.
Mouth Taping Affects HRV
HRV (heart rate variability) is a commonly used measure of the body’s recovery and resilience. It is the variation in time between heartbeats, reflecting the balance between the sympathetic and parasympathetic nervous system. Higher HRV is generally considered better. It’s an indicator of how well you adapt to stress.
Right now, our data shows that the average participant experiences a 2ms increase in HRV when taping. Pretty cool! This effect seems to be more pronounced for mouth breathers (+5ms) than nose breathers (+1ms, maybe?).
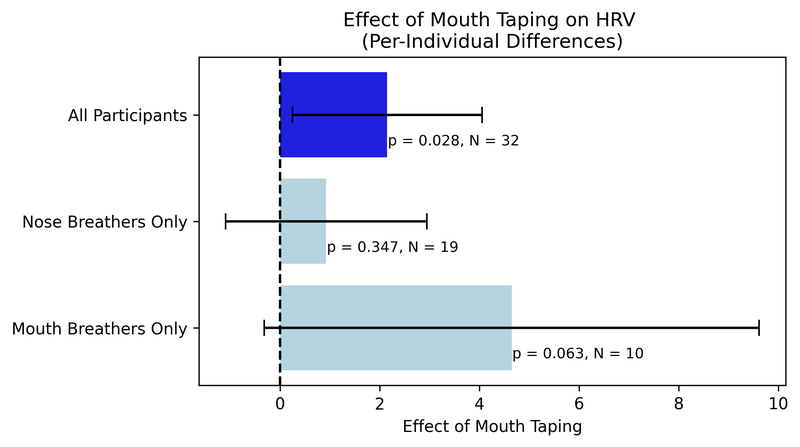
Is 2ms a lot though? That’s like moving up 0.4 standard deviations in the population – e.g. from the 50th percentile to the 66th. Would you feel the difference of that effect size?
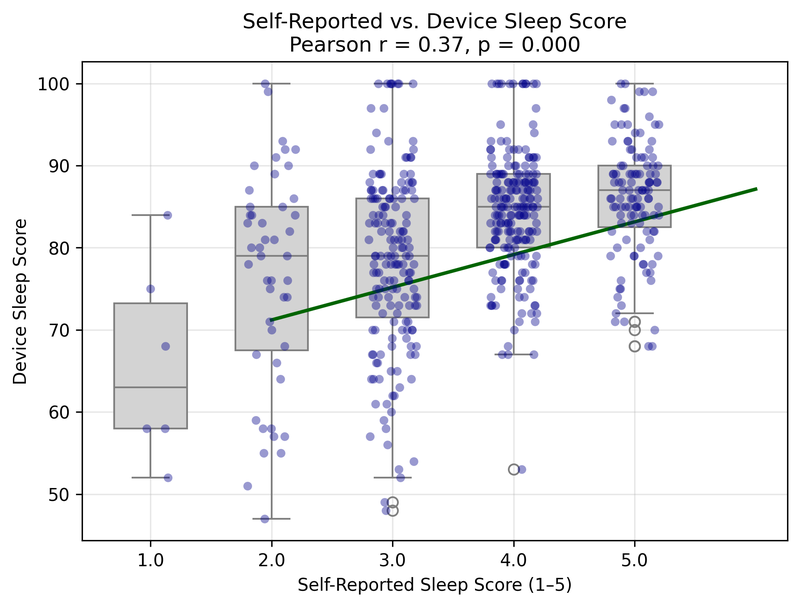
In our data, self-reported sleep scores correlate with device sleep scores. This makes sense, and it’s good to see the subjective data align with the objective measurement.
But when we look at HRV instead of the device’s overall sleep score (which aggregates several sleep metrics), there is basically no correlation between HRV and self-reported sleep quality.
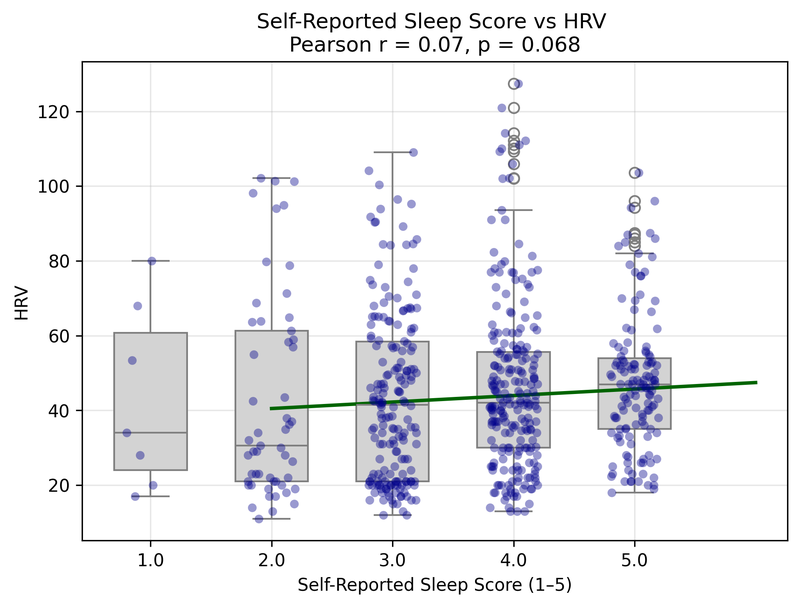
There are multiple ways to interpret this. One possibility is that the device sleep scores include other metrics that are more influential than HRV to how someone perceives their sleep quality.
Another possibility is that HRV captures a type of recovery that isn’t consciously felt, at least not immediately. Someone’s body might be recovering better even if they don’t feel like they slept better.
This is the true opportunity of science: to detect what is not immediately obvious. Measurement tools and specialized experiments help us isolate previously unclear phenomena. Sometimes we confirm what we already know, but other times we uncover something unexpected, something that we wouldn’t have been able to see with just subjective reports from TikTokers and health influencers.
More Data Wanted!
Let’s not jump to conclusions yet. We’ve currently got enough data to include 43 of our participants in this piece of analysis (some metrics may have more or less data available, depending on what was tracked). It’s surprising and exciting that we’re seeing some effects with that, but there’s plenty that we still don’t know.
With more data, the confidence intervals get tighter. We can plot our estimate and the 95% confidence interval around it over time. For example, here is our best estimate of the effect of mouth taping on total sleep time:
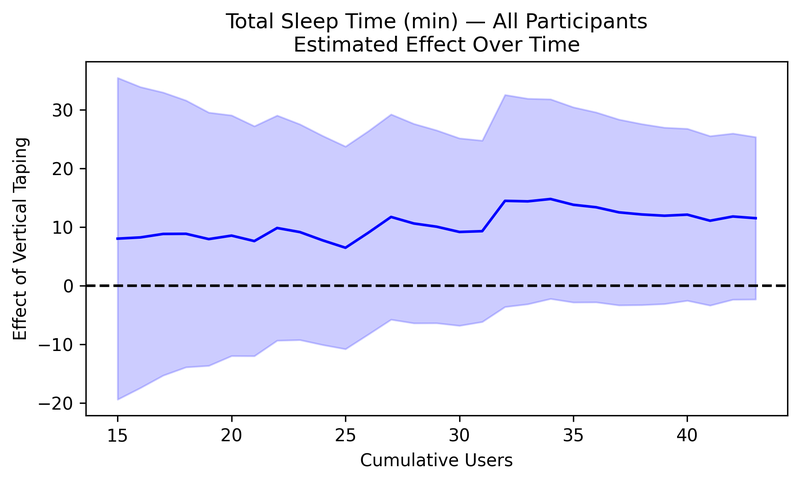
At first, the effect could have been anything from -20 min to +30 min (the initial range of the purple area representing the 95% confidence interval). Over time, we have gotten greater confidence that the effect is positive. Total sleep time might significantly increase from mouth taping, but with 43 participants’ data, we still can’t say for sure (p=0.1101).
As independent researchers, we have the flexibility to keep this study open indefinitely, as we are not bound by academic calendars and grant deadlines. We want more data so that we can be confident not just that an effect exists, but how large and meaningful it truly is. With each additional participant, our estimates become more precise, and we have clearer evidence to share with interested parties.
Other Potentially Interesting Findings
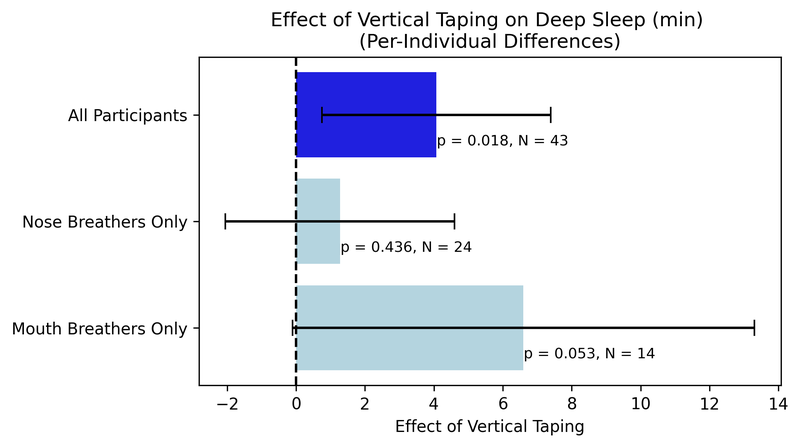
Deep Sleep Time
The average participant's deep sleep time increased by about 4 minutes when vertical taping, and this effect is significant. The effect seems to be more pronounced in mouth breathers than in nose breathers.
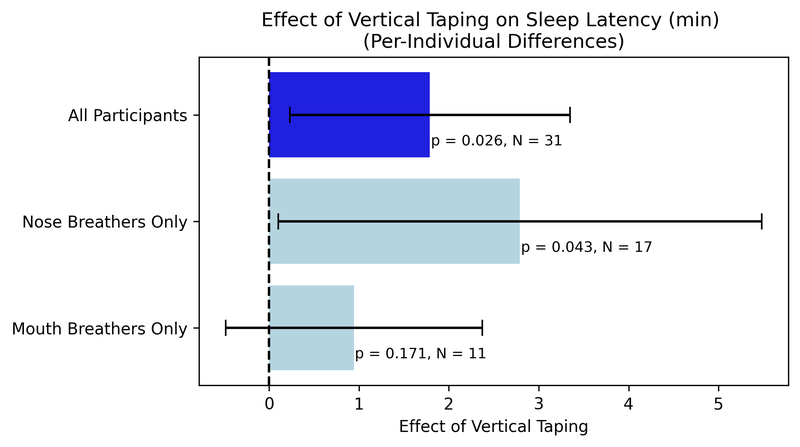
Sleep Latency
The average participant takes longer to fall asleep with vertical tape, with sleep latency increasing by about 2 minutes. Perhaps it is uncomfortable to fall asleep with tape on, especially as one gets used to it.
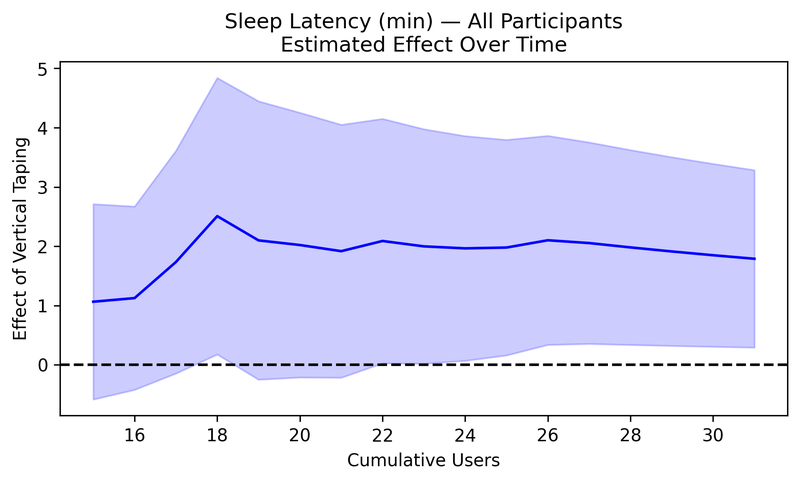
The estimated effect on sleep latency has remained pretty consistent and became statistically significant after about 24 participants.
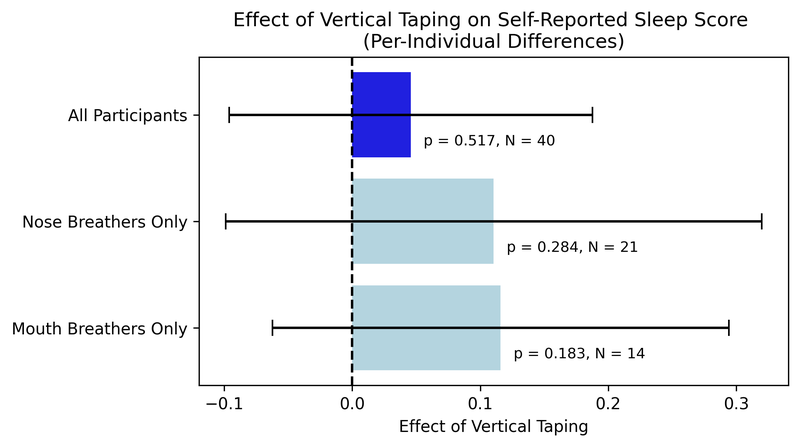
Self-Reported Sleep Score
In general, the effects of mouth taping are not subjectively apparent.
There’s more to this story, and we need your help to figure it out. Share these early findings, talk about the study, or better yet: join in yourself. The more data we collect, the clearer the picture becomes.
All participants receive a personalized report of their outcomes, an Amazon gift card for the tape, a prize raffle for a new Apple Watch Series 10, and the glory of supporting groundbreaking biohack mythbusting (or fact-validating).
This study is independent, ongoing, and transparent. We're not selling anything, just trying to figure out what's true. Huge thanks to Anton for conceptualizing and supporting this project.
Onboarding form here.